What Does Interoperability Mean for Medical Equipment?
- Qubit Technology
- 3 days ago
- 9 min read

When a patient is wheeled into the ICU, a dozen devices start collecting data simultaneously. The question of what does interoperability mean for medical equipment becomes life-or-death specific: can those devices actually talk to each other, share that data meaningfully, and feed it into clinical decisions without a nurse manually transcribing numbers? Most healthcare professionals hear “interoperability” and think connectivity. That’s the first misconception worth correcting. True interoperability in healthcare is a four-layer problem spanning technical protocols, data formats, shared clinical meaning, and organizational governance. Understanding all four layers changes how you buy, deploy, and manage medical equipment.
Table of Contents
Key Takeaways
Point | Details |
Interoperability has four layers | Foundational, structural, semantic, and organizational layers must all be addressed for meaningful data exchange. |
Standards form the technical backbone | IEEE 11073 and HL7 FHIR are the core standards that govern device-to-device and system-level communication. |
Integration is not interoperability | Integration merges systems into fixed infrastructure; interoperability lets systems communicate while staying autonomous. |
Semantic depth is the hardest part | Sharing data is not enough; systems must share the meaning of data using terminologies like SNOMED CT and LOINC. |
Procurement decisions carry interoperability risk | Selecting equipment without assessing standards compliance creates costly, dangerous connectivity gaps downstream. |
What does interoperability mean in medical equipment, defined in four layers
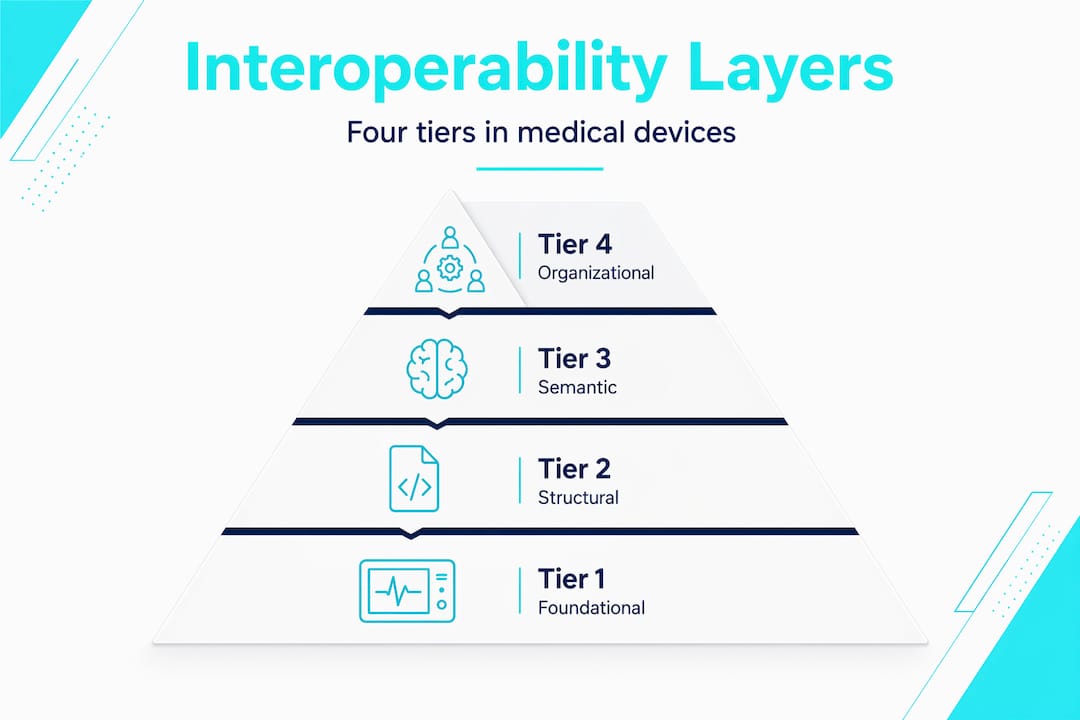
The four-layer framework for medical equipment interoperability covers everything from raw signal transmission to the policies that govern data use. Each layer builds on the one below it, and a failure at any layer breaks the chain.
Here is how the layers break down:
Foundational interoperability: The device can send data to another system. This is basic transport. Think TCP/IP packets from a ventilator reaching a gateway server. No guarantees about format or meaning.
Structural interoperability: The data arrives in a standardized format that the receiving system can parse. HL7 messages and FHIR resources are examples. The system knows where the heart rate field is located.
Semantic interoperability: The receiving system understands what the data means, not just where it sits. This requires shared clinical terminologies. A glucose reading coded with LOINC means the same thing in your EHR as it does in a remote monitoring platform.
Organizational interoperability: The policies, governance frameworks, and workflow agreements that allow different institutions or departments to use exchanged data effectively and legally.
Layer | Example | Key Standard or Mechanism |
Foundational | Pulse oximeter transmits SpO2 over Wi-Fi | TCP/IP, MQTT |
Structural | EHR parses the SpO2 value from an HL7 message | HL7 v2, FHIR R4/R6 |
Semantic | System recognizes SpO2 LOINC code as peripheral oxygen saturation | SNOMED CT, LOINC |
Organizational | ICU protocol specifies when SpO2 data triggers an alert workflow | HIPAA policies, IHE profiles |
Pro Tip: When evaluating new devices, ask vendors specifically which layer their compliance claims cover. A device that is “FHIR-compliant” may only achieve structural interoperability without also supporting validated LOINC or SNOMED CT bindings.
Critically, consistent terminology mapping using codes like SNOMED CT and LOINC is what separates systems that technically exchange data from those that actually communicate meaning. Most organizations overestimate how far they have gotten because they stop measuring at layer two.
Core standards and technologies that make it work
Understanding the standards stack is not just an IT department concern. If you are a clinical director, department head, or procurement lead, this is the layer where your equipment choices either create long-term flexibility or lock you into costly workarounds.
The two dominant standards are IEEE 11073 and HL7 FHIR. IEEE 11073 and HL7 FHIR serve different but complementary roles. IEEE 11073 governs point-of-care device communication, defining how bedside monitors, infusion pumps, and diagnostic devices encode and transmit physiological data at the device level. FHIR (Fast Healthcare Interoperability Resources) operates at the system level, providing RESTful API-based data exchange between EHRs, clinical applications, and device management platforms.
FHIR is evolving quickly. The DeviceAlert resource in FHIR R6 standardizes how clinical device alarms are communicated between systems. Previously, alarm data from infusion pumps or ventilators was modeled inconsistently across vendors. DeviceAlert replaces ad hoc approaches and enables unified alarm management at the EHR level. That is a significant clinical safety improvement.
IHE (Integrating the Healthcare Enterprise) profiles sit above these individual standards and define how they work together in specific clinical scenarios, like how a device connects to an EMR during a patient care episode. They provide the workflow-level interoperability layer that raw standards do not address on their own.
The reality on the ground is messier. No single standard suffices in a multi-vendor environment. Legacy devices may only support HL7 v2 or proprietary protocols, while modern systems expect FHIR R4 or R6. This is where middleware and integration engines come in. Products like Rhapsody or Mirth Connect translate between older protocols and modern FHIR interfaces, but they add complexity and maintenance overhead.
Pro Tip: When issuing an RFP for new medical equipment, include explicit requirements for IEEE 11073 compliance and FHIR R4 or R6 support. Request documentation on how the vendor handles legacy protocol bridging if you are running a mixed environment.
For healthcare providers working with IT partners on HIPAA-compliant data transfer, the transport layer also matters for security. RESTful APIs over HTTPS, MQTT with TLS for IoT devices, and certificate-based authentication are not optional in regulated environments.
Integration vs. interoperability: why the distinction matters
These two terms get used interchangeably, and that habit costs organizations money and creates clinical risk. They are fundamentally different approaches with very different consequences.
Integration merges systems into rigid infrastructure, while interoperability enables flexible, secure data exchange while each system stays autonomous. An integrated environment might require all devices to connect through a single vendor’s proprietary hub, creating dependency and making it difficult to swap out components. An interoperable environment lets a new imaging device from one manufacturer communicate directly with an EHR from another, without requiring a full system rebuild.
Here is why the distinction matters operationally:
Scalability: Interoperable systems can accommodate new devices without redesigning the entire infrastructure.
Vendor independence: You are not locked into one vendor’s ecosystem for upgrades or replacements.
Clinical workflow continuity: Autonomous systems can be updated, replaced, or expanded without taking down connected workflows.
Error reduction: When devices communicate through standardized interfaces rather than bespoke integrations, there are fewer custom code points where data can be lost or corrupted.
The organizational layer of interoperability, including governance policies, access controls, and workflow protocols, is what makes the technical exchange clinically useful. Data landing in an EHR without a defined workflow for acting on it creates noise, not value. Successful implementations focus on workflow bottlenecks rather than raw data exchange volume.
Pro Tip: Before deploying any new medical device integration project, map the clinical workflow it is supposed to support first. Technology should solve a specific care coordination or documentation problem, not generate data that clinicians do not have protocols to act on.
Implementation challenges and how to address them
Knowing the definition of interoperability is the easy part. Getting there in a real healthcare environment is where most organizations struggle.
Challenge | Recommended Practice |
Protocol diversity across legacy and modern devices | Deploy middleware or integration engines to translate between HL7 v2 and FHIR |
Inconsistent clinical terminology use | Implement a clinical terminology server for centralized SNOMED CT and LOINC mapping |
ISO 14971 risk gaps for connectivity hazards | Document latency, message loss, and update error scenarios during device development |
EHR-agnostic connectivity failures | Use a validated, structured device connectivity architecture like Oracle’s program |
Staff and governance readiness | Align IT, clinical, and compliance teams before technology deployment |
The most overlooked challenge is risk management. Interoperability failures often stem from neglecting connectivity hazards during product development. Under ISO 14971, manufacturers are required to address risks like message latency, data loss during network interruption, and incorrect value updates. When these are skipped, safety incidents follow, along with expensive post-market remediation.
The semantic layer is where most organizations hit their ceiling. Dedicated terminology service infrastructure is critical because FHIR transport compliance alone does not guarantee that two systems interpret data the same way. A FHIR-compliant device sending a medication dose still needs both sending and receiving systems to map that dose to the same drug code in a shared terminology. Without a terminology server handling that mapping consistently, you have structural interoperability without semantic interoperability.

Pro Tip: If your organization is mid-deployment and discovering terminology mismatches, prioritize a centralized terminology server before adding more devices to the network. Fixing semantic gaps retroactively is far more expensive than building the infrastructure once, correctly.
Emerging trends and the real-world value of interoperability
The payoff for getting interoperability right is substantial and measurable. The most tangible recent example comes from AI-driven platforms. Platforms with unified real-time patient journeys can cover up to 75% of a hospital’s patient population, enabling AI-powered clinical decision support across care settings. That only works when device data flows freely and meaningfully into the algorithms.
Real-world benefits for healthcare systems that achieve true interoperability include:
Faster time to treatment through automated early warning systems fed by device data
Reduced redundant testing when lab and imaging results are accessible across care settings
Better risk stratification for high-acuity patients through combined data streams
Stronger regulatory compliance, since regulatory frameworks increasingly require documented interoperability and data integrity claims as part of device approval
Improved care coordination between inpatient and outpatient teams sharing the same patient record in real time
When selecting equipment with interoperability in mind, evaluate vendors on four criteria: standards compliance documentation (specifically IEEE 11073 and FHIR version), terminology support, legacy bridging capability, and post-market update transparency. The last point matters more than most buyers realize. A device that is FHIR R4 compliant today but has no upgrade path to R6 will need replacing sooner than expected, particularly as DeviceAlert and other new resources become standard expectations.
For facilities looking at leading surgical equipment options, selecting equipment from vendors who publish their interoperability roadmaps is a concrete way to reduce procurement risk.
My take: interoperability is a safety issue, not a feature
I’ve spent years watching healthcare organizations treat interoperability as a box to check during procurement, something handled by the IT department while clinicians focus on care delivery. That separation is expensive and, at times, dangerous.
Here is the uncomfortable truth: most healthcare facilities are operating at layer one or two of the interoperability framework while believing they have solved the problem. They have devices that connect. They have HL7 messages moving. But the semantic layer, the part where your sepsis algorithm and your EHR agree on what a white blood cell count means in a specific clinical context, is still broken. And when it breaks, clinicians compensate manually. They copy and paste. They re-enter data. They develop workarounds that introduce new error pathways.
What I’ve learned is that the organizations that achieve genuine interoperability treat it as a risk management and patient safety priority from day one. Not as a vendor feature to be negotiated during procurement. They build governance structures before they buy equipment. They map clinical workflows before deploying integrations. They ask harder questions of vendors than most RFPs require.
The practical reality is also this: you do not have to solve everything at once. Prioritizing the clinical areas where data fragmentation is causing the most harm, usually ICU, emergency, and surgical settings, and fixing those first delivers measurable patient outcomes while building institutional competency for the harder semantic and organizational layers.
— QB
Find the right supplies for your interoperable clinical environment
Building an interoperable clinical environment requires more than the right software stack. The physical supplies and equipment in your facility need to meet the same standards of reliability and compliance that your data infrastructure demands. Queenssurgical serves hospitals, clinics, and healthcare facilities across the Americas with high-quality medical supplies that meet rigorous industry standards. From surgical masks with certified protection to essential clinical instruments, Queenssurgical’s catalog is built for practitioners who need dependable, competitively priced solutions. Explore the full range at Queenssurgical and see how the right supplier partnership supports the safe, effective clinical environments that interoperable care demands.
FAQ
What does interoperability mean for medical equipment?
Interoperability in medical equipment means devices and systems can exchange, interpret, and act on shared data meaningfully. It spans four layers: technical transport, standardized formats, shared clinical terminology, and organizational governance.
How is interoperability different from integration?
Integration merges systems into a single fixed infrastructure, while interoperability allows separate systems to communicate freely while remaining autonomous. Interoperability offers greater scalability and vendor independence than traditional integration approaches.
What standards govern medical device interoperability?
IEEE 11073 governs point-of-care device communication, and HL7 FHIR handles system-level data exchange through RESTful APIs. IHE profiles define how these standards work together in specific clinical workflows.
Why is semantic interoperability the hardest layer to achieve?
Semantic interoperability requires all systems to share the same meaning for clinical data, not just the same format. Without a clinical terminology server mapping codes like SNOMED CT and LOINC consistently, FHIR-compliant systems can still misinterpret each other’s data.
How does interoperability affect patient outcomes?
Interoperable systems reduce redundant testing, accelerate early warning responses, and improve care coordination between clinical teams. Platforms achieving broad patient population coverage enable AI-driven clinical decision support that directly improves treatment speed and accuracy.
Recommended
Comments