What Is Consignment Inventory Medical? A 2026 Guide
- Qubit Technology
- Jun 7
- 9 min read

Medical consignment inventory is stock physically placed at a healthcare provider’s site but owned by the supplier until consumed, with billing triggered only at the point of use. This model is standard practice for high-value, low-predictability items like orthopedic implants, surgical kits, and cardiovascular devices. For hospital administrators and procurement teams, understanding how consignment inventory works in healthcare means understanding a supply arrangement that protects cash flow, improves clinical availability, and introduces a distinct set of compliance obligations. This guide covers the full picture: operational workflows, financial and legal implications, comparisons with traditional and vendor-managed inventory, and the management practices that separate high-performing programs from costly ones.
What is consignment inventory in medical settings?
Medical consignment inventory, formally called a consignment stock arrangement, is a supply model where the vendor retains legal ownership of goods stored at your facility until a clinical event consumes them. The hospital does not pay for the item until it is used on a patient. That single principle separates consignment from every other procurement model in healthcare.
The most common examples are orthopedic implant trays, cardiac stents, and surgical instrument sets. A spine surgeon may need one of six implant sizes during a procedure. The hospital cannot predict which size in advance, so the supplier places the full tray on-site. Only the implant actually used triggers an invoice. The remaining items stay on the supplier’s balance sheet, not the hospital’s.

Consignment shifts cost burdens and improves clinical availability, but it creates a trust-based partnership that demands explicit management rules. Without those rules, the model that was designed to reduce financial risk becomes a source of billing disputes, expired waste, and audit failures.
How does the medical consignment process work in practice?
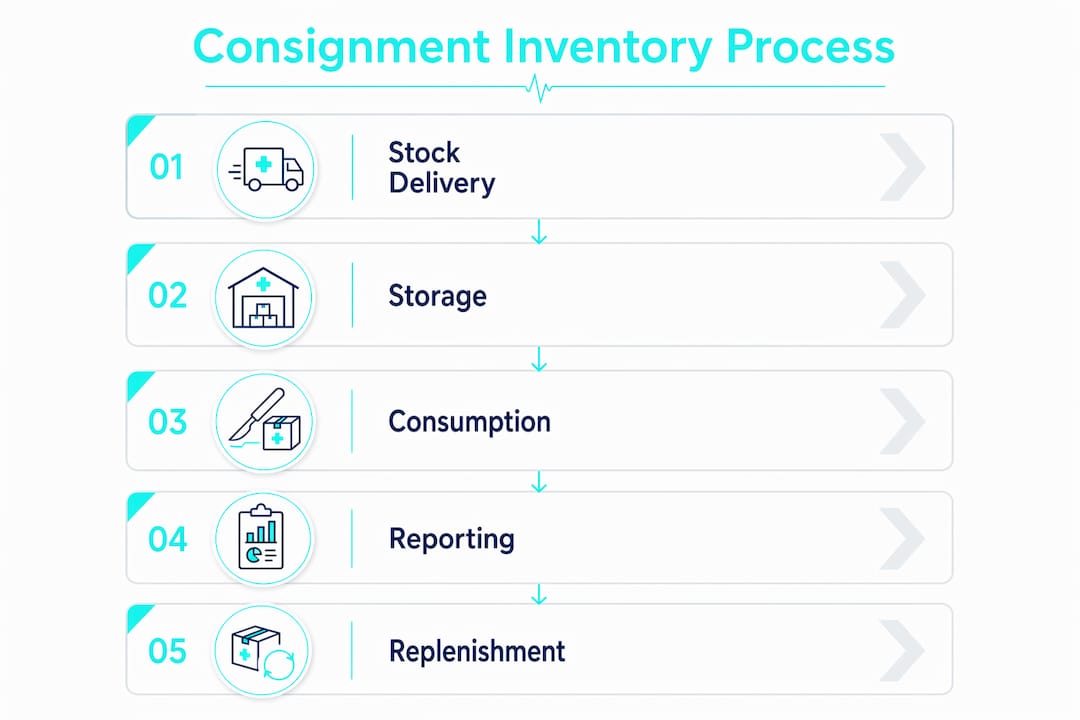
The medical consignment process follows a defined sequence from vendor delivery to replenishment. Understanding each step helps you identify where your current workflow may be losing money or creating compliance exposure.
Stock placement. The supplier delivers consigned goods to your facility, typically a storeroom, surgical suite, or cath lab. Ownership stays with the supplier. Your team receives the items but does not record a purchase.
Point-of-consumption trigger. A clinician uses the item. This event, not delivery, is what transfers ownership and initiates billing. Scan-to-use workflows complete this step in 5 to 10 seconds at the point of care using a barcode or RFID scan.
Automated replenishment. Once usage drops stock below a pre-agreed par level, the system sends a replenishment alert or automatically generates a purchase order to the supplier. This keeps clinical availability high without manual reordering.
Invoice generation. The consumption event triggers an invoice for the specific item used, including its UDI (Unique Device Identifier) and lot number. Finance receives a clean, traceable record tied to a specific patient case.
Audit and reconciliation. Periodic physical counts reconcile on-hand stock against system records. Discrepancies reveal shrinkage, expired items, or documentation gaps.
Inventory management software is the operational backbone of this process. Platforms like SAP operationalize consignment as special document types for fill-up, pick-up, and billing on consumption, which supports correct invoicing and prevents the manual errors that cause disputes.
The most common operational failure is delayed consumption reporting. Delayed or manual reporting triggers mismatched inventory records, billing disputes, and compliance failures. If your team documents usage on paper and enters it into a system hours or days later, you are carrying the risk of every gap in between.
Pro Tip: Assign a single point of accountability per clinical area for consumption documentation. Diffuse responsibility is the primary reason scan-to-use compliance rates drop below 80% in high-volume surgical suites.
What are the financial and compliance implications?
Consignment inventory preserves hospital liquidity because payment is due only on consumption, not on delivery. For high-cost implantable devices, this can represent a significant reduction in working capital tied up in on-hand stock. That financial benefit comes with legal and regulatory obligations that many facilities underestimate.
Legal ownership under U.S. commercial law. Consignment agreements in the U.S. intersect with UCC Article 2-326, which governs consignment sales. Without a UCC-1 financing statement filed by the supplier, consigned goods may be claimed by hospital creditors in a bankruptcy proceeding. Suppliers who skip this filing lose their ownership protection. Hospitals should understand this dynamic because it affects how contracts are structured and what documentation your legal team should request.
FDA and EU MDR traceability requirements. The FDA requires UDI capture for Class II and Class III devices. In Europe, EUDAMED compliance from May 28, 2026 requires traceability for consignment devices including UDI and lot number capture at the point of use. Manual tracking creates direct regulatory risk. Software-based capture at consumption is no longer optional for facilities handling consigned implantables.
Key financial and compliance risks to monitor:
Shrinkage rates of 5 to 15% are common without real-time consumption data. That range represents direct financial loss shared between supplier and hospital depending on contract terms.
Expired inventory costs fall to whichever party the contract assigns them. Facilities without automated expiry alerts routinely absorb costs that should have triggered a supplier return.
Billing disputes arise when consumption records do not match supplier invoices. The root cause is almost always a documentation lag, not a disagreement on price.
Consignment terms must avoid inducement risk through fair market value pricing. Par levels tied to projected volume increases can trigger Anti-Kickback Statute scrutiny in the U.S.
Consignment inventory preserves hospital liquidity but creates cross-functional risks for medtech companies and their hospital partners that require disciplined tracking and audit trails. Finance, legal, and clinical operations must all be aligned on the same contract terms and the same system of record.
Consignment vs. traditional and vendor-managed inventory
Three models dominate medical supply management: traditional stocked inventory, consignment, and vendor-managed inventory (VMI). Each solves a different problem, and confusing them creates process failures.
Model | Ownership at delivery | Who manages replenishment | Payment timing |
Traditional stocked inventory | Hospital | Hospital | At delivery |
Consignment inventory | Supplier | Shared or supplier | At consumption |
Vendor-managed inventory (VMI) | Hospital | Supplier | At delivery or agreed terms |
The critical distinction is that VMI focuses on who manages replenishment, while consignment focuses on who owns the stock until use. A hospital can have VMI without consignment (supplier manages reorders, but hospital owns the stock on arrival) or consignment without VMI (supplier owns the stock, but hospital manages its own reorders). Most modern programs combine both: the supplier owns the stock and manages replenishment. That combination is where the operational complexity concentrates.
For a deeper look at how VMI applies to healthcare supply chains, the distinctions between ownership and replenishment responsibility become especially important when auditing existing supplier agreements.
Traditional inventory is the simplest model to manage but the most capital-intensive. You own everything on the shelf from the moment it arrives. Consignment reduces that capital burden but requires more sophisticated tracking. VMI reduces your administrative workload on reordering but does not change your ownership position unless combined with consignment terms.
Pro Tip: Review every supplier agreement in your current portfolio and classify it explicitly as traditional, consignment, or VMI. Mixing these models in a single storage location without clear labeling is the leading cause of audit failures in hospital supply rooms.
Best practices for managing medical consignment inventory effectively
Effective consignment inventory management in healthcare requires coordination across procurement, finance, clinical operations, and compliance. The following practices reflect what separates programs that generate value from those that generate disputes.
Define contract terms with precision. Every consignment agreement should specify par levels, usage reporting timelines, ownership transfer triggers, expiry return policies, and shrinkage liability. Vague contracts are the primary source of billing disputes. For guidance on structuring procurement agreements, wholesale purchasing frameworks offer useful structural parallels.
Implement scan-to-use at every consumption point. Barcode or RFID scanning at the point of care eliminates documentation lag. Pair this with software that automatically updates inventory records and triggers replenishment alerts. Facilities using inventory management tips from healthcare logistics specialists consistently report fewer billing discrepancies.
Conduct regular physical audits. Reconcile system records against physical counts at least quarterly. For high-value implantables, monthly counts are standard. Audits catch shrinkage early and provide the documentation trail regulators expect.
Separate consigned stock from owned stock physically and systematically. Consignment implemented like standard stocking causes audit failures due to confusion over ownership timing and inventory mixing. Use dedicated storage locations, clearly labeled bins, and separate system flags for consigned items.
Align finance and clinical staff on consumption documentation. Finance cannot reconcile invoices if clinical staff do not document usage in real time. Cross-functional training on why accurate consumption data matters reduces the gap between clinical practice and financial accuracy.
Monitor expiry dates actively. Automated expiry alerts allow your team to return items before they expire, avoiding costs that would otherwise fall to the hospital. This is especially relevant for biologics and single-use devices with short shelf lives.
For facilities managing storage compliance alongside consignment tracking, reviewing medical equipment storage requirements provides a useful framework for maintaining regulatory alignment across both dimensions.
Key takeaways
Medical consignment inventory creates measurable financial and operational advantages for hospitals only when ownership, documentation, and compliance obligations are managed with the same rigor as clinical protocols.
Point | Details |
Ownership transfers at consumption | The supplier owns consigned stock until a clinical event triggers use, billing, and ownership transfer. |
Scan-to-use is the operational standard | Real-time barcode or RFID capture at point of care eliminates documentation lag and billing disputes. |
EUDAMED and FDA require UDI capture | From May 2026, traceability for consigned devices including lot numbers is a regulatory requirement, not optional. |
VMI and consignment are distinct models | VMI governs replenishment responsibility; consignment governs ownership. Confusing them causes audit failures. |
Contracts must address shrinkage and expiry | Shrinkage rates of 5 to 15% are common without real-time data. Contract terms must assign liability clearly. |
Why consignment inventory management is harder than it looks
I have seen facilities adopt consignment arrangements for orthopedic implants and treat them operationally like any other stocked item. The implant tray arrives, it goes on the shelf, and someone writes down what was used after the case. That approach works until the first audit, the first billing dispute, or the first EUDAMED inspection. Then it stops working very quickly.
The real challenge with medical consignment is not the concept. Every procurement professional understands that paying after use is better than paying on delivery. The challenge is the cross-functional discipline required to make it work. Finance needs clean consumption data. Legal needs properly filed UCC-1 statements. Clinical staff need a scan-to-use habit that holds under pressure in a busy OR. Compliance needs a traceable audit trail for every device.
What I find most underestimated is the cost of shrinkage. A 10% shrinkage rate on a consignment program covering $2 million in implant inventory is $200,000 in unrecovered cost. That number does not appear on any single line item. It accumulates quietly in billing discrepancies, expired returns, and items that cannot be located during audits.
The facilities that get this right treat consignment as a managed program, not a procurement category. They assign ownership of the program to a specific person, invest in software that captures consumption in real time, and review contract terms annually. For a practical look at how consignment medical equipment retail translates into day-to-day operations, the operational detail is worth reviewing before you expand any existing program.
The competitive advantage for hospitals that master consignment management is real. Lower capital tied up in inventory, higher clinical availability, and cleaner supplier relationships all follow from disciplined execution.
— QB
Stock your facility with reliable supplies from Queenssurgical
Managing consignment inventory well means knowing exactly what you have on hand and where it came from. For the supplies your facility purchases outright, sourcing from a reliable partner removes one layer of complexity from your procurement process.
Queenssurgical supplies hospitals, clinics, and healthcare facilities across the Americas with high-quality medical products at competitive prices. From infection control essentials to procedural consumables, the catalog covers what your team needs without the sourcing delays that disrupt clinical operations. The CPE Thumb Loop Isolation Gown is a practical example: a reliable, competitively priced item that belongs in every facility’s owned inventory alongside any consignment program. Browse the full catalog at Queenssurgical to find products that meet your facility’s standards.
FAQ
What is consignment inventory in healthcare?
Consignment inventory in healthcare is a supply arrangement where the vendor retains ownership of medical goods stored at a hospital or clinic until a clinician uses them, at which point billing is triggered. Common examples include orthopedic implants, surgical kits, and cardiovascular devices.
How does consignment differ from vendor-managed inventory?
Consignment defines who owns the stock until consumption; vendor-managed inventory defines who manages replenishment. A supplier can manage both ownership and replenishment simultaneously, but the two concepts address different aspects of the supply relationship.
What are the main risks of medical consignment inventory?
The primary risks are shrinkage of 5 to 15% without real-time tracking, billing disputes from documentation lag, expired inventory costs, and regulatory non-compliance if UDI and lot number capture at point of use is not implemented.
What does EUDAMED require for consignment devices in 2026?
EUDAMED compliance from May 28, 2026 requires traceability for consigned medical devices including UDI and lot number capture at the point of use. Manual tracking systems create direct regulatory exposure under EU MDR.
How should hospitals structure consignment contracts?
Consignment contracts should specify par levels, usage reporting timelines, ownership transfer triggers, expiry return policies, shrinkage liability, and fair market value pricing to avoid Anti-Kickback Statute risk in the U.S.
Recommended
Comments