Retail Medical Compliance Requirements: 2026 Guide
- Qubit Technology
- 4 days ago
- 8 min read

If you think retail medical compliance requirements are a one-time checklist you complete during onboarding and never revisit, you are carrying the most expensive misconception in healthcare administration. The reality is that retail medical compliance spans federal mandates from HIPAA, the Centers for Medicare and Medicaid Services (CMS), the Food and Drug Administration (FDA), and the Drug Enforcement Administration (DEA), each enforced with financial penalties that can threaten your facility’s operational survival. This guide breaks down every critical layer so you can manage compliance as the continuous, living process it actually is.
Table of Contents
Key takeaways
Point | Details |
Compliance is never a one-time event | Retail medical regulations require continuous monitoring, updated risk plans, and recurring staff training. |
HIPAA violations are financially devastating | Average HIPAA fines reach $1.5M, making data protection a financial priority, not just a clinical one. |
DME documentation windows are strict | CMS requires a face-to-face practitioner visit within 6 months before a DMEPOS order is placed. |
Audit trails must be immutable | Write-once audit logs are a regulatory baseline; modified or deleted logs are a major enforcement red flag. |
Telehealth is not less regulated | The same documentation standard required for in-person care applies to all telehealth prescribing and consultation. |
What are retail medical compliance requirements: the federal framework
Retail medical compliance requirements are the legally mandated rules, standards, and operational practices that govern how retail healthcare facilities handle patient data, medical products, billing, and controlled substances. They are not optional guidelines. They are enforceable federal and state obligations with financial, criminal, and operational consequences for non-compliance.
Four federal agencies define the core of this framework:
HIPAA (Health Insurance Portability and Accountability Act): The Privacy Rule, Security Rule, and Breach Notification Rule collectively govern how protected health information (PHI) is collected, stored, transmitted, and disclosed. Retail pharmacies, clinics, and medical supply businesses that handle PHI are covered entities subject to full HIPAA requirements.
CMS Conditions of Participation (CoPs): These are the operational standards facilities must meet to participate in Medicare and Medicaid programs. CMS can deny reimbursements to any facility that fails to meet these conditions, making operational compliance as financially critical as clinical compliance.
FDA 21 CFR Part 11: This regulation governs electronic records and electronic signatures used in pharmaceutical and medical device contexts. Non-compliance can halt operations and expose facilities to warning letters and product holds.
DEA Regulations: Any retail facility that dispenses, stores, or manages controlled substances must comply with DEA scheduling, storage, recordkeeping, and reporting requirements. Violations carry criminal liability, not just fines.
State-level pharmacy boards and health departments add another layer on top of these federal requirements. Licensing, staffing ratios, inspection schedules, and compounding rules vary significantly by state. A medical retail compliance checklist that works in Texas may be incomplete in New York. You must account for both federal floors and state ceilings when building your compliance program.
HIPAA compliance in retail medical settings
HIPAA is where retail healthcare facilities face their most persistent and costly compliance exposure. The average HIPAA fine reaches $1.5M, and that figure does not include remediation costs, reputational damage, or lost patient trust.

The starting point for any serious compliance effort is mapping PHI data flows. You need to know exactly where patient information enters your systems, where it travels, who touches it, and where it exits. Retail pharmacies and clinics often discover during this process that PHI is flowing through systems they had not considered, including scheduling software, third-party billing services, and even text messaging platforms.
From that data flow map, you build your access controls. HIPAA’s minimum necessary standard requires that staff only access PHI relevant to their specific job function. A front-desk employee should not have access to clinical prescription records. An insurance verification specialist should not be able to pull full patient histories.
Pro Tip: Conduct quarterly access rights audits rather than waiting for annual reviews. Staff roles change frequently in retail medical settings, and stale access permissions are among the most common HIPAA findings during enforcement investigations.
Here is a structured sequence for building HIPAA compliance in retail contexts:
Complete an enterprise-wide HIPAA risk analysis covering every system, device, vendor, and employee that touches PHI.
Document your risk management plan with named owners and specific deadlines for each identified risk.
Execute Business Associate Agreements (BAAs) with every vendor, software provider, and contractor who accesses PHI on your behalf.
Implement administrative safeguards: written policies, workforce training, designated privacy officers.
Implement physical safeguards: locked workstations, restricted server access, secure document disposal.
Implement technical safeguards: role-based access controls, automatic logoff, and encryption.
Train all staff at onboarding and annually, with role-specific content rather than generic overviews.
Establish a documented breach response process with clear internal escalation paths.
On breach notification specifically: HIPAA requires notification to affected individuals without unreasonable delay and no later than 60 days after discovering a breach of unsecured PHI. Breaches affecting 500 or more individuals require simultaneous federal notification and media notification in the affected area. Missing this window is itself a separate violation.
Encryption is not optional at this point. Encryption at rest and in transit is now the baseline expectation for PHI protection in any retail healthcare environment.
DME and medical supply compliance requirements
Durable Medical Equipment (DME) and medical supply compliance sits at the intersection of clinical, documentation, and procurement requirements. If your facility orders, supplies, or bills for DME, DMEPOS (Durable Medical Equipment, Prosthetics, Orthotics and Supplies) rules apply to you directly.
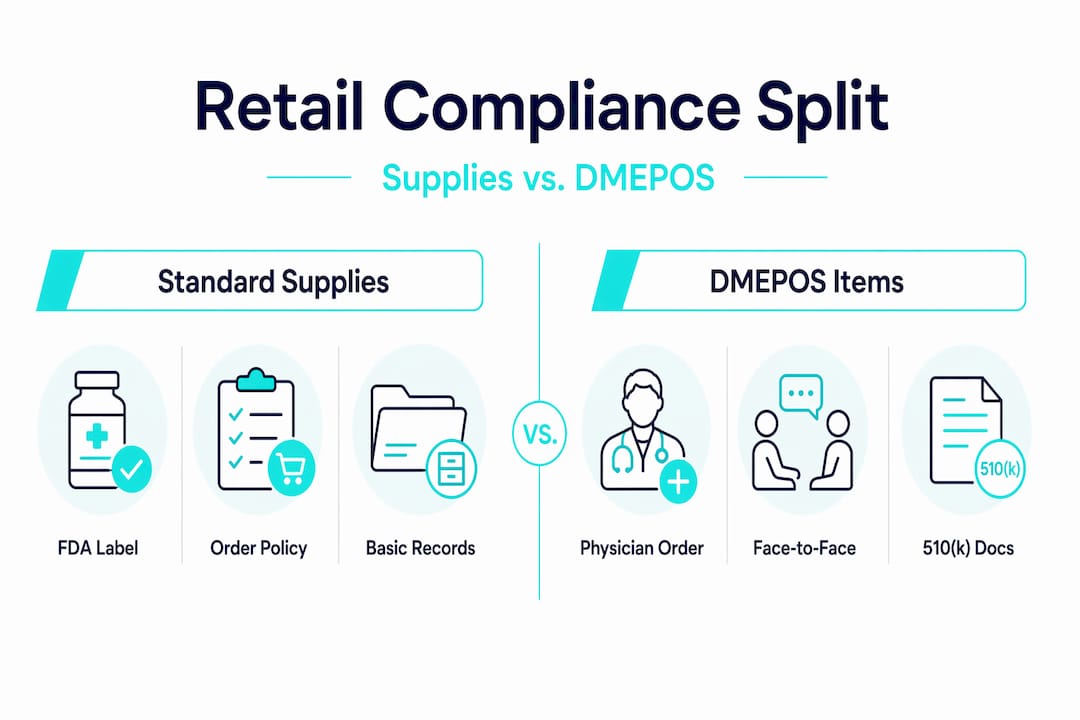
The table below outlines the key compliance differences between standard retail medical supplies and DMEPOS items:
Requirement | Standard medical supplies | DMEPOS items |
Physician order required | Depends on item type | Always required |
Face-to-face encounter | Not required | Required within 6 months of order |
Clinical documentation | Basic usage notes | Full clinical evaluation on record |
FDA labeling compliance | Required | Required plus device classification |
Medicare billing eligibility | Limited | Subject to DMEPOS accreditation |
The face-to-face requirement is where many retail facilities lose Medicare reimbursement. CMS requires that a practitioner visit must occur within 6 months before the DMEPOS order, and that visit must be documented with a clinical evaluation supporting the medical necessity of the equipment. An order written without this documentation will be denied on audit.
FDA labeling compliance is a separate but equally critical requirement for medical supply retailers. Every product you sell or distribute must carry accurate, approved labeling that matches its FDA clearance or approval status. Advertising claims for medical devices must not exceed what the device’s clearance permits.
Pro Tip: When onboarding new suppliers, request copies of FDA 510(k) clearance letters or premarket approval documentation as part of your vendor qualification process. This protects you from distributing mislabeled or unapproved products. Learning how consignment medical equipment retail operates can also clarify your distribution obligations under federal law.
Operational compliance strategies that actually work
Building a compliance program that holds up under audit requires more than written policies. 5.3% of pharmacy service standards were rated as “not met” or “requiring improvement” in a recent two-year regulatory review across 77 pharmacy inspections. That failure rate exists despite most facilities having compliance documentation in place. The gap is always in execution.
Here is what operationally mature compliance programs do differently:
Formalize the program structure. Appoint a dedicated compliance officer with authority to escalate issues directly to leadership. Compliance cannot live inside a single department or be treated as an add-on to another role.
Conduct scheduled internal audits. Do not wait for regulators to find problems. Run your own mock audits against CMS, HIPAA, and DEA requirements at least twice per year, and document every finding and remediation.
Maintain immutable audit trails. Write-once audit log patterns are required to demonstrate data integrity during investigations. Any evidence of deleted or modified logs is treated as a major red flag by regulators, and rightfully so.
Address telehealth compliance explicitly. A common misconception is that telehealth prescribing is less regulated than in-person care. In practice, the same standard of care and documentation is required. Automated questionnaires without documented clinical decision-making are among the most common enforcement targets in 2026.
Conduct regular security risk assessments. Technology environments change faster than compliance frameworks. New software, devices, and remote work arrangements each create fresh PHI exposure points that your risk analysis must capture.
Pro Tip: When handling a regulatory audit or voluntary disclosure, do not attempt to manage the response ad hoc. Pre-designate a response team, identify your outside counsel in advance, and run a tabletop simulation at least once per year so everyone knows their role before it matters.
When ordering medical supplies online, build supplier verification into your procurement process. Confirm that vendors maintain proper FDA registration, provide compliant documentation, and can supply chain-of-custody records on request.
My take on where retail medical compliance actually fails
I’ve reviewed compliance programs across retail pharmacy, clinic, and medical supply environments, and the pattern is consistent. Facilities invest in building the framework and then treat it as finished. The policy binder gets updated once a year if someone remembers to schedule it. The risk analysis gets filed after the first assessment and not revisited until something goes wrong.
What I’ve found is that compliance culture is the variable most correlated with audit outcomes. When compliance is genuinely embedded into daily workflows rather than bolted on as a reporting exercise, staff catch problems before they become violations. They ask questions. They flag unusual requests. They do not need to be reminded to log off their workstations.
The uncomfortable truth is that technology, which most vendors sell as the compliance solution, can actually create compliance debt if it is not governed properly. New software introduces new PHI exposure. Automated telehealth platforms create documentation gaps when they substitute questionnaire responses for clinical judgment. State medical boards have become increasingly aggressive about enforcement precisely because the technology has outpaced the oversight.
My practical advice: treat your compliance program like your clinical quality program. Give it real resources, real ownership, and real accountability. Regulations do not stay still, and neither should your response to them.
— QB
How Queenssurgical helps you source with confidence
Compliance does not stop at your policies and procedures. It extends to every product that enters your facility, from the gloves on your clinicians’ hands to the labeling on your sample vials. That supply chain integrity is where Queenssurgical adds direct operational value.
Queenssurgical supplies medical facilities across the Americas with products that meet industry quality standards, from nitrile examination gloves to specialized labeling supplies essential for sample management and regulatory documentation. Every product category is sourced to support healthcare providers who need reliable, specification-accurate supplies without the procurement complexity. Whether you are restocking a retail pharmacy, equipping a clinic, or managing a DME operation, Queenssurgical’s catalog is built around what compliance-conscious facilities actually need. Visit Queenssurgical to browse the full catalog and request supply documentation to support your compliance records.
FAQ
What are retail medical compliance requirements?
Retail medical compliance requirements are the federal and state mandates governing how retail healthcare facilities manage patient data, medical products, billing, and controlled substances. The primary frameworks include HIPAA, CMS Conditions of Participation, FDA 21 CFR Part 11, and DEA regulations.
How often must a HIPAA risk analysis be updated?
HIPAA does not specify a fixed interval, but regulators expect facilities to update their risk analysis whenever significant changes occur in systems, vendors, or operations, and at minimum annually. A documented, enterprise-wide assessment covering all systems and vendors is required.
What documentation is required before ordering DMEPOS items?
CMS requires a practitioner face-to-face encounter within 6 months before the DMEPOS order, with clinical evaluation documentation supporting medical necessity. Orders placed without this documentation are subject to denial or recoupment on audit.
Does telehealth reduce the documentation burden for retail medical providers?
No. The same standard of care and clinical documentation required for in-person encounters applies to telehealth. Automated questionnaires without documented clinical judgment are among the most common enforcement targets for state medical boards and CMS reviewers in 2026.
What is an immutable audit trail and why does it matter?
An immutable audit trail is a log of system activity recorded with write-once technology that cannot be altered or deleted after the fact. Regulators treat any evidence of modified or deleted audit logs as a major compliance violation under both HIPAA and FDA 21 CFR Part 11.
Recommended
Comments