Medical Equipment Maintenance Schedule for Hospitals
- Qubit Technology
- Jun 6
- 9 min read

A medical equipment maintenance schedule is a structured plan that defines specific maintenance tasks, responsible personnel, and service intervals to keep medical devices performing safely and reliably. Hospitals and clinics that operate without a formalized schedule risk device failures, failed accreditation surveys, and patient safety incidents. Standards like The Joint Commission EC.02.04.01, ISO 13485, and frameworks such as the Oxmaint preventive maintenance checklist give healthcare administrators a proven foundation for building a schedule that satisfies regulators and protects patients.
What is a medical equipment maintenance schedule?
A medical equipment maintenance schedule is the operational backbone of any biomedical engineering program. It specifies which devices get inspected, what tasks are performed, how often, and by whom. Without this structure, maintenance becomes reactive rather than planned, and reactive maintenance costs more and fails more often.
The schedule typically organizes tasks into four tiers: daily, monthly, semi-annual, and annual. Daily tasks cover operational readiness and alarm function checks. Monthly tasks address calibration verification and mechanical integrity. Semi-annual tasks include electrical safety testing, and annual tasks require full device certification with technician sign-off and corrective action documentation. This tiered structure prevents task overlap and makes workload distribution manageable for biomedical teams.

Regulatory frameworks reinforce this structure. The Joint Commission EC.02.04.01 requires facilities to maintain a complete equipment inventory, set inspection intervals based on risk, and document every maintenance activity to pass accreditation surveys. ISO 13485 adds quality management requirements that align maintenance records with device lifecycle documentation. Together, these standards define the minimum bar your schedule must clear.
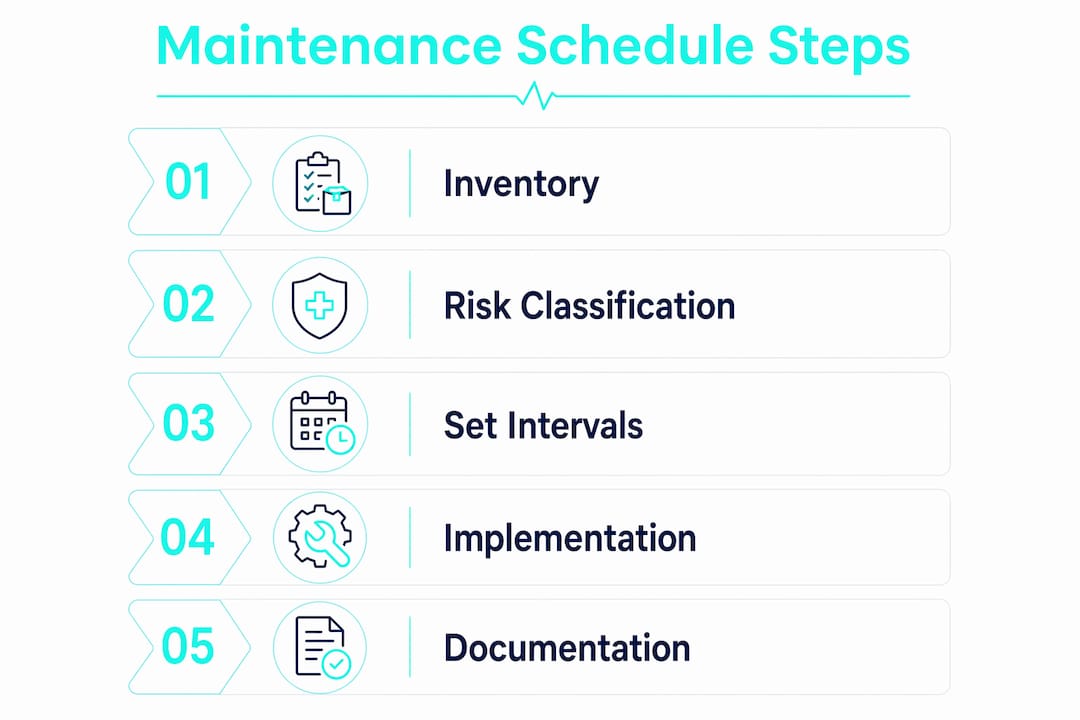
What you need before building your schedule
Before you write a single maintenance interval, you need three things in place: a complete equipment inventory, a risk classification system, and access to manufacturer documentation.
Your inventory is the foundation. Every device your facility owns or leases must appear in the register, tagged with a unique asset ID, location, device type, and current status. Facilities that manage medical equipment storage requirements alongside their inventory records reduce the risk of missing devices during audits. Without a complete inventory, your schedule will have gaps, and gaps become compliance failures.
Risk classification determines how often each device gets serviced. The Joint Commission uses a risk assessment scoring matrix that scores equipment on function, physical risk, required maintenance type, and incident history. Scores drive frequency tiers, from quarterly maintenance for life-support devices to annual checks for non-critical equipment. Applying this matrix before you set any intervals prevents both over-maintenance of low-risk devices and under-maintenance of critical ones.
Manufacturer instructions for use (IFU) and service manuals provide the baseline intervals your schedule must start from. Regulatory bodies treat manufacturer recommendations as the default, and any deviation requires formal justification. Gather these documents for every device in your inventory before you open a scheduling tool.
Pro Tip: Create a shared digital folder organized by asset ID that stores the IFU, service manual, and risk score for each device. When a technician or auditor needs documentation, retrieval takes seconds instead of hours.
Finally, choose your scheduling platform before you build. A computerized maintenance management system (CMMS) like UpKeep, Limble CMMS, or IBM Maximo automates work order generation, tracks completion rates, and stores records in one place. A spreadsheet-based system works for smaller facilities but creates traceability risks as device counts grow.
How to set maintenance intervals that actually hold up
Setting intervals is a risk-management process, not a calendar exercise. The right starting point is always the manufacturer’s recommended interval. From there, you adjust based on three inputs: device criticality, usage volume, and field performance history.
Follow this sequence when establishing or revising intervals:
Start with manufacturer baseline. Record the manufacturer-recommended interval for every device. This is your default and your legal starting point.
Apply risk tier adjustments. High-criticality devices (ventilators, infusion pumps, defibrillators) warrant shorter intervals regardless of manufacturer guidance. Low-criticality devices may qualify for extended intervals under a formal program.
Review field performance data. Calibration drift records, repair logs, and failure history tell you whether the current interval is working. A device that consistently drifts before its scheduled calibration needs a shorter interval.
Document any deviation formally. Interval optimization is recognized by regulators as sound practice, provided you document the risk assessment and performance data that justify the change.
Implement an AEM program if needed. Alternative Equipment Maintenance programs allow deviation from manufacturer intervals when supported by detailed risk assessments. Under TJC standards, AEM programs require a 100% maintenance completion rate and thorough documentation to withstand regulatory scrutiny.
Set utilization-based triggers where applicable. Calibration and inspection schedules improve when you add utilization triggers alongside calendar dates. A high-volume ultrasound unit used 200 times per month needs different treatment than one used 20 times.
Pro Tip: Build a simple interval review log that records the original manufacturer interval, the current facility interval, the justification, and the date of last review. Auditors respond well to facilities that can show a documented decision trail rather than just a number in a spreadsheet.
Hospitals must achieve a 100% maintenance completion rate for scheduled tasks to satisfy The Joint Commission. That target is only achievable if your intervals are realistic. Intervals set too aggressively create a backlog that technicians cannot clear. Intervals set too loosely create compliance and safety risk. The goal is a schedule your team can actually execute.
Step-by-step process for implementing your schedule
Once your inventory, risk scores, and intervals are set, implementation follows a clear sequence. The table below maps each phase to its core deliverable.
Phase | Action | Deliverable |
1. Register and classify | Enter all devices into CMMS with asset ID, location, and risk tier | Complete, tagged equipment inventory |
2. Build task checklists | Create frequency-specific checklists for daily, monthly, semi-annual, and annual tasks | Standardized task lists per device category |
3. Assign and schedule | Assign technicians, generate work orders, set due dates | Active work order queue |
4. Execute and document | Technicians complete tasks, record results, and sign off digitally | Traceable service records |
5. Review and update | Audit completion rates and adjust intervals or resources as needed | Continuously improved schedule |
Checklist design matters more than most administrators realize. Task-driven checklists aligned to frequency tiers outperform generic device checklists because they focus the technician on the right tasks at the right time. A monthly checklist for an infusion pump looks different from its annual checklist, and both should be distinct documents in your system.
Digital tools change the execution dynamic significantly. A CMMS generates work orders automatically, sends reminders before due dates, and flags overdue tasks in real time. Proactive work order generation based on utilization and device drift trends can prevent overdue maintenance and reduce reactive repairs during staffing shortages or high clinical demand. That capability alone justifies the investment for most mid-size hospitals.
Best practices for documentation and regulatory compliance
Documentation is where most facilities lose accreditation surveys. A well-designed schedule means nothing if the service records cannot prove it was executed.
Every service record must capture four elements: device identity (asset ID and serial number), tasks performed, results and measurements, and technician sign-off with credentials. Linking these records to the device’s full asset history creates the traceability chain auditors look for. Facilities frequently fail audits due to incomplete service record chains that cannot connect device identity, test instruments used, tasks performed, and technician sign-off.
For software-enabled devices, the bar is higher. Electronic service records must comply with FDA QMSR and 21 CFR Part 11, including pre- and post-service test results, software version changes, device configuration, and verification signatures. This is not optional for connected devices, and it is increasingly relevant as hospitals add more networked equipment.
“The operational difference between a checklist-based maintenance program and a survey-ready system is completeness and traceability of all inspection and maintenance activities.” — Joint Commission Maintenance Compliance Guide
Preparing for a Joint Commission survey means more than having records. You need to demonstrate that your schedule covers every device in inventory, that completion rates are at or near 100%, and that any interval deviations are backed by documented risk assessments. Facilities that align their regulatory compliance processes with their maintenance documentation workflows reduce survey preparation time significantly.
Common documentation pitfalls include missing technician credentials on service records, incomplete corrective action notes, and service records stored in disconnected systems that cannot be retrieved quickly during a survey. Audit your documentation quarterly, not just before a scheduled survey.
Common challenges and how to solve them
Even well-designed schedules run into execution problems. The most frequent obstacles fall into three categories: interval adherence, resource constraints, and justification gaps.
Missed maintenance windows. The most common cause is an overloaded work order queue. Solve this by auditing your interval assignments against available technician hours. If your team cannot realistically complete the schedule, the schedule needs adjustment, not the team.
Interval justification conflicts. When a manufacturer recommends quarterly calibration but your field data supports semi-annual, you need a defensible AEM program. Reducing maintenance frequency without a defensible AEM program risks non-compliance. Document the risk analysis before you change the interval.
Operational downtime conflicts. Scheduling maintenance on devices that clinical teams need continuously requires coordination. Build maintenance windows into device scheduling systems so clinical staff know when a device will be unavailable.
Technician compliance gaps. Incomplete task execution often traces back to unclear checklists or inadequate training. Standardize checklists, conduct quarterly technician reviews, and use CMMS completion data to identify patterns.
Pro Tip: Involve charge nurses and department heads in scheduling discussions. Clinical teams that understand why maintenance windows exist are far more cooperative than those who see maintenance as an interruption. A 15-minute monthly briefing builds more goodwill than any policy memo.
My take on what actually separates good programs from great ones
After working closely with healthcare procurement and clinical operations teams, the pattern I see most often is this: facilities invest in the schedule design but underinvest in the documentation infrastructure. They build a solid checklist, assign technicians, and then store records in three different systems that no one can search during a survey.
The facilities that consistently pass Joint Commission surveys without scrambling are the ones that treat documentation as part of the maintenance task itself, not as an administrative afterthought. Their technicians close work orders in the CMMS before they leave the room. Their asset histories are complete. Their interval justifications are filed next to the device record.
I also think the industry underestimates how much medical equipment interoperability matters for maintenance programs. When your CMMS talks to your clinical IT systems, you get utilization data that makes interval optimization genuinely data-driven rather than a best guess. That integration is worth pursuing even if it requires IT project time.
The other thing I would push back on is the instinct to start with the most complex devices. Start with your highest-volume, mid-criticality devices. You will build process discipline faster, your team will gain confidence, and you will have a working model to apply to life-support equipment.
— QB
Keep your maintenance program stocked and ready with Queenssurgical
A maintenance schedule only works when your team has the right supplies on hand when they need them. Technicians performing equipment inspections and cleaning procedures need reliable disposable protective wear to maintain hygiene standards and prevent cross-contamination between devices.
Queenssurgical supplies hospitals and clinics across the Americas with the disposable medical supplies that support daily maintenance routines. From disposable lab uniforms designed for fluid resistance and latex-free safety to disposable suction canisters that support clinical equipment upkeep, Queenssurgical makes it easy to order what you need at competitive prices. Browse the full catalog at queenssurgical.net and keep your maintenance program fully equipped.
Key takeaways
A medical equipment maintenance schedule requires a complete inventory, risk-based interval setting, and traceable documentation to satisfy The Joint Commission and protect patient safety.
Point | Details |
Start with inventory and risk scores | Every device needs an asset ID, location, and risk tier before you set a single interval. |
Use four frequency tiers | Daily, monthly, semi-annual, and annual task tiers keep workloads manageable and audits clean. |
Document every deviation | Any interval change from manufacturer guidance requires a formal AEM program with supporting data. |
Prioritize traceability | Service records must link device ID, tasks performed, test results, and technician sign-off. |
Automate with a CMMS | Digital work order systems prevent missed maintenance and generate the audit trail regulators require. |
FAQ
What is a medical equipment maintenance schedule?
A medical equipment maintenance schedule is a structured plan that assigns specific inspection and service tasks to defined intervals (daily, monthly, semi-annual, annual) for every device in a facility’s inventory. It ensures devices perform safely, supports regulatory compliance, and reduces unplanned failures.
How often should medical equipment be serviced?
Service frequency depends on device criticality, manufacturer recommendations, and risk assessment scores. Life-support devices typically require quarterly or more frequent maintenance, while low-risk equipment may qualify for annual service under a documented AEM program.
What does The Joint Commission require for equipment maintenance?
The Joint Commission EC.02.04.01 requires a complete equipment inventory, risk-based inspection intervals, and fully documented service records. Facilities must demonstrate a 100% maintenance completion rate during accreditation surveys.
What records are required for medical device maintenance?
Each service record must include the device asset ID, tasks performed, measurement results, technician credentials, and sign-off date. Software-enabled devices also require pre- and post-service test results and software version documentation to comply with FDA QMSR and 21 CFR Part 11.
What is an Alternative Equipment Maintenance program?
An AEM program allows a healthcare facility to deviate from manufacturer-recommended maintenance intervals when supported by formal risk assessments and documented field performance data. Under TJC standards, AEM programs require 100% maintenance completion and thorough documentation to remain compliant.
Recommended
Comments