Medical Equipment Lifecycle Explained for Healthcare Administrators
- Qubit Technology
- Jun 9
- 8 min read

Medical equipment lifecycle management is the structured discipline of tracking every device from purchase through decommission, with a focus on ownership status, physical condition, and replacement timing. Understanding what is medical equipment lifecycle explained in practical terms means recognizing that every piece of clinical equipment follows a defined path through procurement, active use, maintenance, and eventual disposal. Each phase generates data that directly shapes patient safety outcomes, regulatory compliance, and capital budget decisions. Facilities that manage this process formally spend significantly less per device and experience fewer unplanned equipment failures than those that operate reactively.
What are the key stages of the medical equipment lifecycle?
The medical equipment lifecycle stages follow a structured sequence that begins before a device arrives on the floor and continues long after it stops being used clinically. Each stage has distinct goals, activities, and data outputs that feed into the next phase.
Stage 1: Procurement and commissioning. This phase covers vendor selection, purchase, delivery, and the critical step of acceptance testing. Commissioning establishes the baseline measurements that every future inspection will be compared against. Missing this baseline creates a complete gap in condition trending, making it nearly impossible to detect gradual performance degradation later.

Stage 2: Active use and preventive maintenance. This is the longest phase and the most resource-intensive. Clinical staff operate the device daily while biomedical engineers execute scheduled preventive maintenance (PM) tasks, calibration checks, and corrective repairs. Every work order generated here becomes a data point for future replacement decisions.
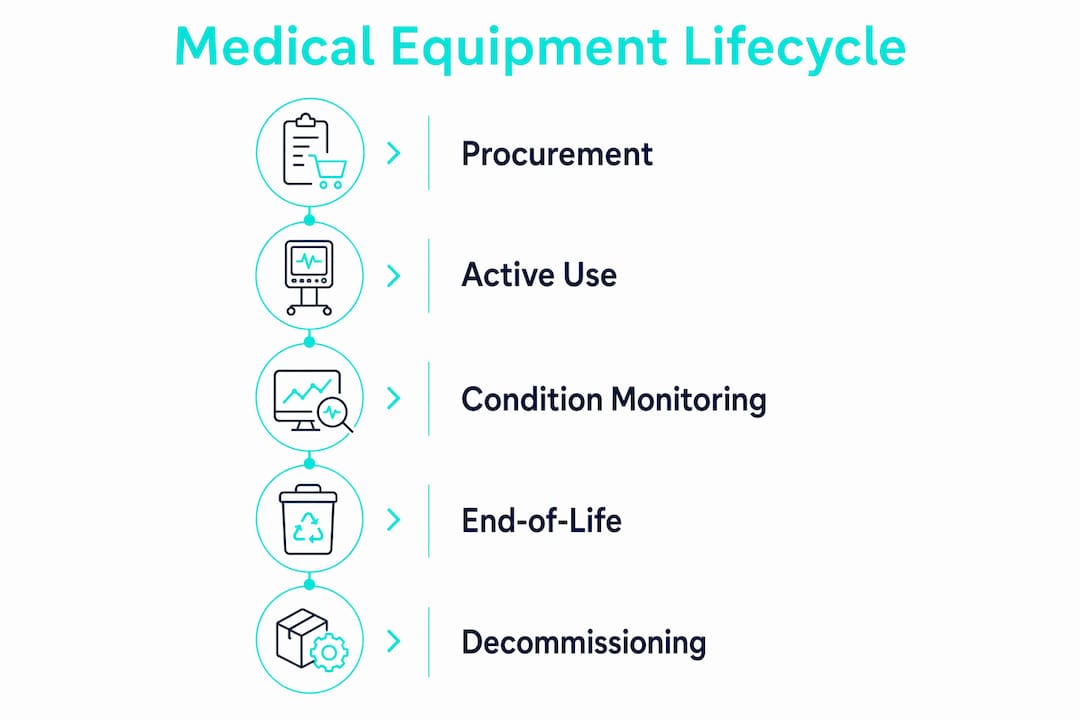
Stage 3: Condition monitoring and performance trending. Rather than waiting for a device to fail, condition monitoring uses repair frequency, calibration drift, and wear rate data to identify declining performance before it becomes a safety issue. This is where structured programs separate themselves from reactive ones.
Stage 4: End-of-life planning and capital forecasting. When condition data signals that a device is approaching the end of its useful life, the replacement cycle begins. This phase involves multi-year capital expenditure (CapEx) planning, vendor negotiations, and scheduling clinical downtime for the transition.
Stage 5: Decommissioning and disposal. The device is formally removed from the asset register, data is wiped if applicable, and physical disposal follows regulatory requirements. Regulations like WEEE (Waste Electrical and Electronic Equipment) and biohazard handling protocols govern this step depending on device type.
Pro Tip: Document acceptance testing results in your computerized maintenance management system (CMMS) on the day of commissioning. That baseline record is the single most valuable data point in the entire lifecycle.
How do healthcare facilities manage the active use and maintenance phase?
The active use phase accounts for 78% of lifecycle costs, driven by preventive maintenance labor, replacement parts, and corrective repairs. Managing this phase well is the difference between predictable operational budgets and constant financial surprises.
Effective management in this phase depends on balancing two types of maintenance:
Preventive maintenance (PM): Scheduled tasks performed at manufacturer-specified or regulatory-required intervals. PM tasks include lubrication, filter replacement, calibration, and safety checks. These tasks keep devices operating within specification and satisfy Joint Commission on Accreditation of Healthcare Organizations (JCAHO) and FDA requirements.
Corrective maintenance: Unplanned repairs triggered by device failure or performance degradation. Corrective maintenance is unavoidable, but its frequency and cost are controllable through strong PM programs.
Condition trending: Linking each work order to the specific asset record and tracking metrics like mean time between failures (MTBF) and repair cost per device. This turns raw maintenance activity into a predictive tool.
Regulatory compliance tracking: Maintaining documentation that proves PM tasks were completed on schedule. Audit readiness depends entirely on the quality of this record-keeping.
Facilities that rely on inspection due dates alone as their primary management signal lose up to 95% of useful lifecycle data contained in calibration drift, repair histories, and wear patterns. That data loss directly undermines safe replacement timing and cost forecasting.
Pro Tip: Set your CMMS to flag any device that has required three or more corrective repairs within a 12-month period. That threshold often signals the beginning of accelerated decline and gives you 12 to 18 months of lead time for budget planning.
Clinical engineering teams at large health systems like Mayo Clinic and Cleveland Clinic use integrated CMMS platforms to link PM schedules, work orders, and condition scores to individual asset records. Smaller facilities can replicate this approach with platforms like IBM Maximo, Accruent, or UpKeep, scaled to their device inventory size.
Why is end-of-life planning and capital forecasting critical?
Replacement budgeting planned 2 to 3 years in advance using a 5-year CapEx forecast is the standard for facilities that avoid emergency procurement costs. Emergency procurement carries an average 22% price premium over planned purchases, and that figure does not account for the clinical disruption caused by unplanned equipment downtime.
The table below compares planned versus reactive end-of-life management across the metrics that matter most to administrators:
Factor | Planned replacement | Reactive replacement |
Procurement cost | Standard market price | Up to 22% premium above market |
Clinical downtime | Scheduled, minimized | Unplanned, disruptive |
Compliance documentation | Complete and audit-ready | Often incomplete or rushed |
Budget predictability | High, multi-year visibility | Low, unpredictable spikes |
Vendor negotiation leverage | Strong, time allows comparison | Weak, urgency limits options |
Formal decommissioning is more than physically removing a device from service. It requires updating the asset register, completing disposal documentation, and following applicable regulations. WEEE compliance governs electronic waste disposal across many jurisdictions, while devices that contacted biological materials require biohazard handling protocols before disposal or resale. Skipping these steps creates audit exposure and potential liability.
Decommissioning documentation also feeds directly back into the next procurement cycle. The repair history, total cost of ownership, and failure mode data from a decommissioned device inform vendor selection and specification requirements for its replacement. Facilities that treat disposal as a data collection opportunity continuously improve their procurement decisions.
What data and documentation are essential for lifecycle management?
Comprehensive asset records capturing purchase price, warranty terms, maintenance schedules, condition scores, and replacement projections are the foundation of defensible lifecycle decisions. Without this data, replacement decisions default to guesswork or political pressure from clinical departments.
The minimum data set that should be captured at commissioning for every device includes:
Purchase price, vendor name, and contract terms
Warranty start and end dates, including what is covered
Manufacturer-specified PM schedule and task list
Acceptance testing results and baseline performance measurements
Unique asset identifier linked to all future work orders
Expected useful life and projected replacement year
Baseline acceptance testing is the most frequently skipped step in this list, and its absence creates a 100% gap in condition trending. You cannot measure degradation without a starting point. A ventilator that passes acceptance testing at 98% tidal volume accuracy gives you a reference point. If that same device reads 91% accuracy three years later, you have objective evidence of decline. Without the baseline, that 91% reading is meaningless in isolation.
Calibration records, repair work orders, and parts replacement logs must all be linked to the specific asset identifier rather than stored in general department files. This linkage is what allows condition trending and MTBF calculations. ConnectedMedics and similar healthcare professional networks increasingly provide forums where biomedical engineers share documentation templates and CMMS configuration practices that support this kind of structured data capture.
How does lifecycle management benefit administrators and patient care?
Structured medical device lifecycle management produces measurable outcomes across financial, operational, and clinical dimensions. Hospitals managing equipment reactively spend up to 3.1 times more per device annually than those with formal preventive maintenance programs. That cost difference, multiplied across hundreds of devices in a typical acute care facility, represents a material budget impact.
The practical benefits for healthcare administrators and clinical teams include:
Capital budget accuracy: Multi-year CapEx forecasts grounded in condition data replace annual guesswork with defensible projections that finance teams can plan around.
Reduced equipment downtime: Proactive replacement scheduling minimizes the unplanned outages that disrupt clinical workflows and delay patient care.
Audit and regulatory readiness: Complete maintenance records and disposal documentation satisfy JCAHO, FDA, and state health department requirements without last-minute scrambling.
Patient safety improvement: Devices replaced before failure eliminate the risk of mid-procedure equipment malfunction, which is a direct patient safety benefit.
Cross-functional alignment: Lifecycle data creates a shared language between clinical, biomedical, and financial teams, reducing the friction that typically surrounds capital equipment requests.
Pro Tip: Present your 5-year equipment replacement forecast to finance leadership alongside total cost of ownership data for aging devices. Administrators who frame replacement requests in financial terms rather than clinical preference win budget approvals at a significantly higher rate.
Understanding the importance of medical equipment lifecycle management also means recognizing that procurement decisions made today create the maintenance and replacement obligations of the next decade. Choosing equipment from vendors with strong service networks, available spare parts, and clear end-of-life support timelines reduces total lifecycle cost even when the initial purchase price is higher.
The case for treating lifecycle management as a strategic function
Most healthcare facilities I have observed treat equipment lifecycle management as a technical function owned entirely by the biomedical engineering department. That framing is the single biggest obstacle to getting it right.
The commissioning baseline step is almost universally underinvested. Biomedical teams are often under pressure to get new devices into clinical service quickly, and acceptance testing gets abbreviated or its results go undocumented in any structured system. That shortcut costs facilities enormously over a 10-year device lifespan because every subsequent condition assessment lacks a reference point.
End-of-life planning is the other chronically neglected phase. I have seen facilities where the replacement conversation begins only after a device fails in service, at which point the 22% emergency procurement premium is unavoidable and clinical disruption is already happening. A 5-year CapEx forecast built on real condition data changes that dynamic entirely.
The most forward-thinking facilities in 2026 are integrating predictive maintenance signals from connected devices directly into their CMMS platforms, using tools like GE HealthCare’s Centricity or Philips HealthSuite to flag performance anomalies before they become failures. That capability is not exclusive to large health systems. Mid-size facilities with 200 to 500 beds can implement condition-based monitoring for their highest-criticality devices, which typically represent 20% of the inventory but 60% of the clinical risk.
The shift from reactive to proactive lifecycle management is not a technology problem. It is a data discipline problem. Facilities that commit to capturing complete baseline data at commissioning, linking every work order to an asset record, and reviewing condition trends quarterly will outperform those that invest in expensive software but neglect the fundamentals.
— QB
How Queenssurgical supports your equipment procurement needs
Queenssurgical supplies healthcare facilities across the Americas with medical equipment and consumables that meet the quality standards your lifecycle management program depends on. Whether you are in the procurement phase of a new device category or sourcing replacement medical supplies to support active clinical operations, Queenssurgical’s catalog covers instruments, diagnostic equipment, gloves, masks, and wellness products at competitive wholesale and retail pricing. The platform’s B2B purchasing capability makes it practical for hospitals, clinics, and purchasing organizations to source reliably without the delays that inflate emergency procurement costs. Explore Queenssurgical’s full product range and request pricing for your facility’s current procurement cycle.
FAQ
What is medical equipment lifecycle management?
Medical equipment lifecycle management is the structured process of tracking every clinical device from purchase through disposal, covering procurement, active use, maintenance, condition monitoring, end-of-life planning, and decommissioning. Its goal is to maximize device safety, regulatory compliance, and cost efficiency across the full ownership period.
How many stages does the medical equipment lifecycle have?
The medical equipment lifecycle typically includes five to seven stages: procurement and commissioning, active use, preventive maintenance, condition monitoring, end-of-life planning, and formal disposal. Each stage generates data that informs the next phase and supports capital budgeting decisions.
Why does baseline data at commissioning matter so much?
Missing acceptance testing results at commissioning creates a complete gap in condition trending because there is no reference point for measuring performance degradation over time. Without a baseline, condition assessments throughout the device’s life cannot determine whether current performance represents normal wear or accelerating decline.
How far in advance should equipment replacement be budgeted?
Replacement budgeting should begin 2 to 3 years before the projected end-of-life date, supported by a 5-year CapEx forecast. Facilities that plan this far ahead avoid the average 22% price premium associated with emergency procurement and gain time for proper installation planning and clinical transition scheduling.
What regulations govern medical equipment disposal?
Disposal of electronic medical equipment falls under WEEE regulations in many jurisdictions, while devices that contacted biological materials require biohazard handling protocols before disposal or resale. Formal decommissioning documentation is also required to satisfy JCAHO and FDA audit requirements and to update the facility’s asset register accurately.
Recommended
Comments