Medical Consumables vs Durable Equipment: Procurement Guide
- Qubit Technology
- Jun 4
- 8 min read

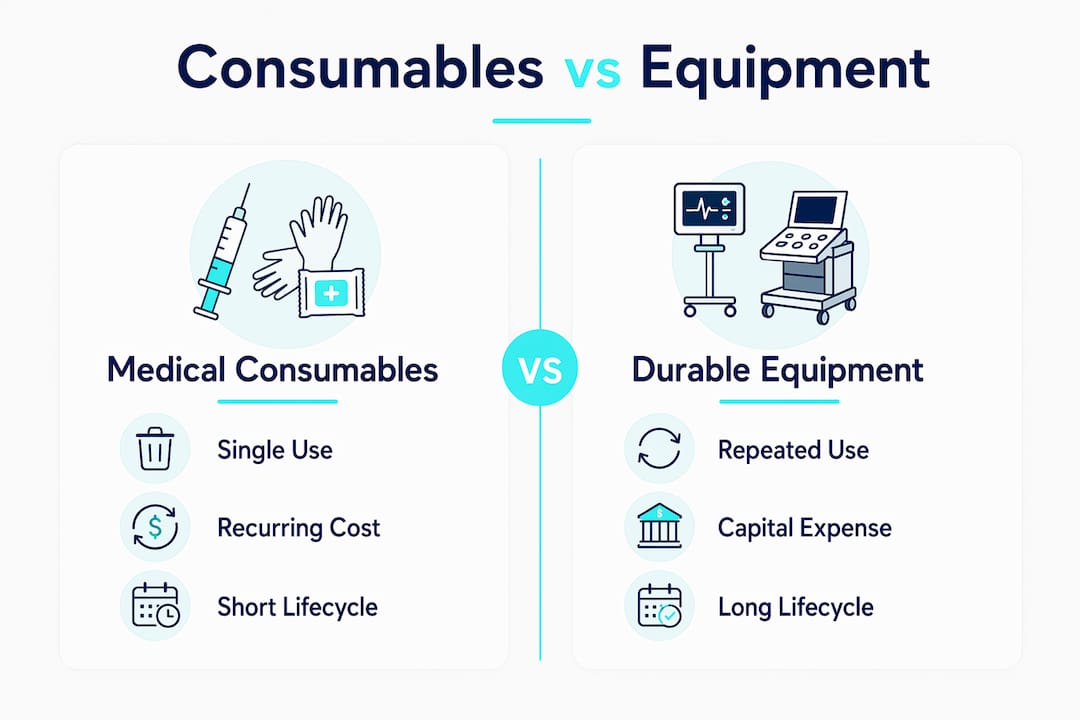
Medical consumables are disposable items used once or over a short period, while durable medical equipment (DME) is designed for repeated, long-term use and typically requires maintenance and calibration. For healthcare professionals and procurement managers, understanding the distinction between medical consumables vs durable equipment determines how you budget, classify, store, and comply with regulatory requirements. The Centers for Medicare and Medicaid Services (CMS), UnitedHealthcare (UHC), and MedCity News each frame this difference as foundational to sound purchasing decisions. Getting the classification wrong costs money and creates compliance exposure.
What are medical consumables and how are they managed?
Medical consumables are single-use or short-term-use items that are discarded after one patient encounter or a brief period of use. Common examples include syringes, wound dressings, alcohol wipes, nitrile gloves, surgical masks, isolation gowns, and urinary catheters. These products are classified as operational expenses on a facility’s budget, not capital assets, which means they do not depreciate and require no maintenance scheduling.
The defining operational challenge with consumables is volume. Procurement teams manage high-volume, recurring inventory that demands constant restocking, accurate demand forecasting, and tight supplier relationships. A single busy surgical unit can burn through thousands of gloves and dressings per week. Shortfalls disrupt patient care directly and immediately.
Key characteristics of medical consumables include:
Single-use design with no expectation of sterilization and reuse
Short shelf life for some categories, requiring first-in, first-out (FIFO) rotation
Hygiene compliance as a non-negotiable, since reusing disposables creates infection risk
No maintenance cost, but significant restocking frequency
High SKU count, often spanning hundreds of product lines across a single facility
Pro Tip: Link your consumables reorder points to actual usage data from your electronic health record (EHR) or inventory management system. Facilities that rely on manual par-level checks consistently over-order low-risk items and under-order high-velocity ones, creating both waste and stockouts simultaneously.
Consumables also appear in the top medical products that retail providers stock most consistently, which reflects their predictable, recurring demand across all care settings.
What defines durable medical equipment: features and lifecycle
Durable medical equipment is defined by CMS and UHC as equipment that is designed for repeated use over months or years and is not consumable or disposable except as needed for effective use. The classification carries direct implications for reimbursement, procurement categorization, and asset management.

Examples of DME include wheelchairs, hospital beds, infusion pumps, ventilators, patient monitors, CPAP machines, and portable oxygen concentrators. These items are treated as capital assets on a facility’s balance sheet, which means they depreciate over time and require structured lifecycle management. A ventilator purchased today will need scheduled preventive maintenance, firmware updates, and eventual replacement planning years from now.
Core characteristics of durable medical equipment include:
Multi-year useful life, often three years or more per Medicare criteria
Maintenance and calibration requirements that generate ongoing service costs
Asset records linking purchase price, warranty, installation date, and maintenance schedules
Higher upfront cost offset by long-term reuse value
Regulatory classification under CMS DMEPOS criteria affecting reimbursement eligibility
Effective asset management requires procurement-to-disposal records that track every stage of the equipment’s life. Facilities that skip this step end up managing DME on spreadsheets, which leads to missed maintenance windows, unexpected failures, and budget surprises.
Pro Tip: At the moment of purchase, create a digital asset record for every piece of durable equipment. Include the purchase price, vendor contact, warranty expiration, preventive maintenance schedule, and expected end-of-life date. This single habit prevents the majority of reactive maintenance crises.
How do consumables and durable equipment compare in cost and procurement?
The most consequential difference between medical consumables vs durable equipment is not the unit price. It is the total cost of ownership across the product’s life. Unit cost is not the same as product cost. Hospitals that evaluate purchases on sticker price alone consistently underestimate the true financial impact of both categories.
The table below captures the core procurement differences:
Factor | Medical consumables | Durable medical equipment |
Usage duration | Single use or short-term | Months to years |
Budget classification | Operating expense | Capital expenditure |
Procurement frequency | Continuous restocking | Periodic replacement |
Maintenance cost | None | Ongoing service and calibration |
Inventory management | High-volume, high-frequency | Asset tracking and lifecycle records |
Regulatory classification | Medical supplies | DMEPOS under CMS criteria |
Insurance/Medicare coverage | Limited, often out-of-pocket | Covered under Part B with documentation |
Consumables generate predictable, recurring spend that compounds over time. A facility spending $0.30 per glove across 10,000 daily patient interactions spends $1.1 million annually on gloves alone. Durable equipment carries a large upfront cost but spreads that investment across years of use. Lifecycle economics drive total cost of ownership far more than the purchase price on any single line item.
Procurement workflows for the two categories also diverge sharply. Consumables procurement runs on demand forecasting, supplier contracts, and inventory turnover metrics. DME procurement runs on capital planning cycles, vendor evaluation, service agreements, and asset lifecycle analysis. Treating them with the same process creates inefficiency in both directions.
Pro Tip: When evaluating a durable equipment purchase, calculate the five-year total cost of ownership: purchase price plus annual maintenance contracts plus consumables the device requires (such as electrodes for a patient monitor or tubing for a ventilator). That number is the real cost.
How do CMS and Medicare DMEPOS policies affect purchasing?
The CMS Master List of DMEPOS items, as of April 13, 2026, includes 530 DMEPOS items that are potentially subject to conditions of payment. A subset of those items requires prior authorization or face-to-face patient encounters before Medicare will reimburse. Misclassifying a product as a consumable when CMS defines it as DME, or vice versa, creates billing errors and potential compliance violations.
The regulatory distinction between consumables and DME affects procurement in three direct ways. First, it determines which budget category absorbs the cost. Second, it determines whether Medicare Part B or another payer covers the item. Third, it determines what documentation your facility must maintain to support a reimbursement claim. Wheelchairs and hospital beds, for example, are durable vs single-use items that illustrate exactly how the reimbursement logic splits.
The consumable vs durable distinction also affects benefit eligibility under commercial payers like UHC, not just Medicare. Procurement managers who understand these classifications can structure purchasing to maximize reimbursement and minimize out-of-pocket exposure for patients and facilities alike.
For facilities operating in regulated retail environments, the 2026 retail medical compliance guide provides a practical framework for aligning purchasing categories with current CMS and payer requirements. Staying current on regulatory changes is not optional. It is a procurement competency.
For facilities managing diabetic supply procurement specifically, understanding diabetic supply payment qualifications in your state adds another layer of compliance precision to consumables purchasing.
Practical integration of consumables and durable equipment in procurement
The most effective procurement strategies treat consumables and durable equipment as interdependent, not separate categories. Many pieces of durable equipment require specific consumables to function. Patient monitors need electrodes. Ventilators need tubing and filters. Infusion pumps need IV sets and administration lines. When the durable equipment ages, consumable demand can spike unexpectedly if procurement analytics do not link inventory data to equipment condition and failure trends.
A practical integration approach follows this sequence:
Map your equipment portfolio by device type, age, and associated consumables. Every piece of DME should have a list of the consumables it requires.
Link consumables reorder triggers to equipment usage data. A ventilator running at high utilization consumes tubing faster than one in standby rotation.
Forecast consumable demand by equipment lifecycle stage. Older equipment often requires more frequent consumable replacement due to wear and compatibility issues.
Coordinate capital and operating budgets. When a major piece of DME approaches end-of-life, budget for both the replacement equipment and the transition-period consumables simultaneously.
Evaluate suppliers on total support capability. A vendor who supplies both the durable equipment and its associated consumables simplifies procurement, reduces SKU fragmentation, and often provides better pricing on bundled contracts.
Healthcare organizations increasingly segment purchasing strategies by using private-label or value-tier options for lower-risk consumables while investing more in premium durable equipment where failure consequences are highest. This approach, highlighted in MedCity News procurement commentary, optimizes cost and performance across the full procurement portfolio rather than applying a single cost-minimization rule to every category.
For facilities exploring alternative acquisition models, understanding consignment equipment retail can reduce upfront capital requirements for DME while maintaining access to current technology.
Key takeaways
The procurement decision between medical consumables and durable medical equipment requires separate budget frameworks, distinct regulatory knowledge, and integrated lifecycle planning to control costs and maintain compliance.
Point | Details |
Classification drives compliance | Misclassifying consumables as DME or vice versa creates billing errors and reimbursement risk under CMS and UHC policies. |
Total cost over unit price | Evaluate durable equipment on five-year total cost of ownership, including maintenance and associated consumables. |
Integrate inventory with equipment data | Link consumables reorder analytics to equipment age and utilization to prevent supply chain gaps. |
Regulatory list is active and specific | The CMS DMEPOS Master List includes 530 items with prior authorization requirements that directly affect procurement workflows. |
Separate procurement processes | Consumables require demand forecasting and restocking contracts; DME requires capital planning and asset lifecycle management. |
Where procurement managers consistently get this wrong
The most common mistake I see procurement teams make is treating the consumables budget and the capital equipment budget as completely separate problems managed by separate people. They are not. Every piece of durable equipment you purchase creates a downstream consumables obligation that will run for years. If the person buying the ventilator and the person managing tubing and filter inventory are not talking to each other, you will have budget surprises every quarter.
The second mistake is assuming that regulatory classification is someone else’s problem, usually billing or compliance. Procurement managers who understand CMS DMEPOS criteria and UHC medical policy make better purchasing decisions from the start. They structure vendor contracts to support documentation requirements. They flag borderline items before they become audit findings rather than after.
The third mistake is evaluating consumables purely on unit price. A cheaper glove that tears more frequently increases staff time, waste, and infection risk. A cheaper wound dressing that requires more frequent changes increases nursing labor cost per patient. The math on “cheaper” consumables almost always looks worse once you account for failure rates and staff workload, exactly as MedCity News frames the sticker-price thinking problem.
The facilities I have seen manage this well share one trait: they have a single procurement framework that treats consumables and DME as two ends of the same supply chain, not two separate departments. That integration is where the real cost control lives.
— QB
How Queenssurgical supports your procurement of consumables and DME
Queenssurgical supplies healthcare facilities across the Americas with the medical consumables that keep durable equipment running and patient care uninterrupted.
From CPE thumb loop isolation gowns and BP cuff barrier sleeves to disposable bedpan covers and fluid-resistant isolation gowns, Queenssurgical stocks the high-volume consumables that procurement managers need on reliable reorder cycles. The platform serves both individual providers and larger purchasing organizations, with competitive pricing and a product catalog built around clinical compliance and infection control standards. If your facility is evaluating consumables suppliers or looking to consolidate SKUs under one trusted source, Queenssurgical is built for exactly that procurement need.
FAQ
What is the main difference between medical consumables and DME?
Medical consumables are single-use or short-term-use items discarded after patient contact, such as gloves and syringes. Durable medical equipment is designed for repeated use over months or years and includes items like wheelchairs, hospital beds, and infusion pumps.
How does CMS classify durable medical equipment vs consumables?
CMS defines DME as equipment expected to be used repeatedly that is not consumable or disposable except as needed for effective use. The CMS DMEPOS Master List currently includes 530 items subject to conditions of payment, with a subset requiring prior authorization.
Does Medicare cover both consumables and durable equipment?
Medicare Part B covers durable medical equipment with proper documentation and physician orders. Most consumables are not covered under Medicare and are treated as operational supply costs absorbed by the facility or patient.
Why does the consumable vs durable classification matter for procurement?
The classification determines budget category (operating expense vs capital expenditure), reimbursement eligibility, documentation requirements, and inventory management strategy. Misclassification creates billing errors and compliance exposure under CMS and commercial payer policies.
How should procurement managers link consumables to durable equipment planning?
Procurement teams should map every piece of durable equipment to its required consumables and link reorder triggers to equipment utilization and age data. As equipment ages, consumable demand often increases, and integrated planning prevents supply chain gaps and budget surprises.
Recommended
Comments