Inventory Turnover for Medical Supplies: 2026 Guide
- Qubit Technology
- 2 days ago
- 8 min read

Inventory turnover in medical supplies is defined as the number of times a healthcare facility sells through and replenishes its entire inventory within a given period, typically one year. This metric, formally called the inventory turnover ratio, is the primary key performance indicator for balancing clinical availability against capital efficiency in healthcare supply chains. The industry benchmark sits at 3–5 turns per year for general healthcare facilities, while high-volume medical-surgical buyers target 4–6 turns annually. Understanding what is inventory turnover for medical supplies, how to calculate it, and how to act on it separates facilities that control costs from those that hemorrhage them.
What is inventory turnover in medical supplies?
Inventory turnover measures how efficiently a healthcare facility cycles through its stock of medical supplies within a set timeframe. A higher ratio generally signals less waste, lower carrying costs, and better cash flow. A lower ratio signals overstocking, potential expiration losses, and tied-up capital that could fund clinical operations.
The standard formula is straightforward: Inventory Turnover = Cost of Goods Sold (COGS) ÷ Average Inventory. Average Inventory equals the beginning inventory value plus the ending inventory value, divided by two. This formula applies directly to medical supply categories including disposables, instruments, and personal protective equipment.

The ratio alone does not tell the full story. A facility running a ratio of 2.0 on surgical gloves is almost certainly overstocked. A facility running 8.0 on a critical implant category is flirting with dangerous stockouts. Context and category matter as much as the number itself.
How to calculate inventory turnover for medical supplies
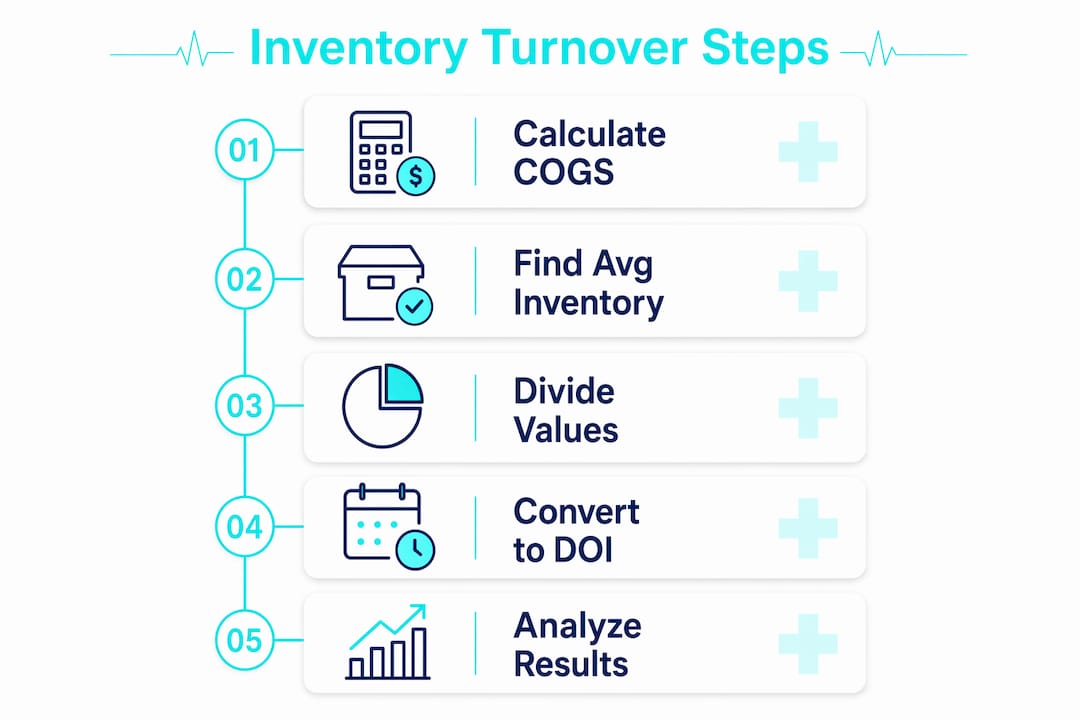
Calculating the inventory turnover ratio for medical supplies follows four clear steps.
Determine your COGS. In healthcare, COGS represents the total cost of medical supplies consumed or sold during the period. This includes disposables like masks, gowns, and gloves, as well as instruments and equipment used in patient care.
Calculate average inventory. Add your beginning inventory value (the dollar amount on hand at the start of the period) to your ending inventory value (the amount on hand at the end). Divide that sum by two.
Apply the formula. Divide COGS by average inventory. For example: if a clinic spent $500,000 on medical supplies in a year and held an average inventory of $125,000, the turnover ratio is 4.0.
Convert to Days of Inventory on Hand (DOI). Divide 365 by the turnover ratio. A 4.0 turnover rate equals approximately 91 days of inventory on hand. This figure tells supply chain managers how long current stock would last if no new orders arrived.
DOI is often more operationally useful than the raw ratio. A supply chain director can act on “we have 91 days of PPE on hand” far more directly than “our ratio is 4.0.”
Pro Tip: Run the DOI calculation separately for each major supply category. A blended facility-wide DOI of 60 days can mask a 200-day DOI on slow-moving items sitting in a back storeroom.
The COGS figure should reflect actual consumption, not purchase orders placed. Facilities that track purchases rather than consumption consistently overstate turnover and underestimate true holding costs.
What are optimal inventory turnover benchmarks for different healthcare settings?
Benchmarks vary significantly by facility type and supply category. Applying a single target across an entire organization produces misleading results.
The table below summarizes industry-standard benchmarks by setting and category type.
Healthcare Setting | Supply Category | Target Turns/Year | DOI Equivalent |
General healthcare facility | All medical supplies | 3–5 | 73–122 days |
High-volume med-surg buyer | Medical-surgical supplies | 4–6 | 61–91 days |
Surgical center | Consumables (gloves, masks) | 6–8 | 46–61 days |
Any facility | High-value implants | 1–3 | 122–365 days |
Any facility | Exam consumables | 6–10 | 37–61 days |
Exam consumables like fast-moving medical supplies turn far faster than high-value implants. Applying the same 4.0 target to both categories will cause you to understock disposables and overstock implants simultaneously.
Calibrating turnover targets by category is not optional. Uniform metrics obscure overstocking of slow-moving items and create risk for critical supplies. A surgical center running 10 turns on nitrile gloves is performing well. A hospital running 10 turns on orthopedic implants has a serious procurement problem.
The 3–5 turns benchmark for general healthcare reflects a balance between avoiding stockouts and avoiding excess carrying costs. Facilities below 3 turns annually are almost certainly holding too much inventory. Facilities above 6 turns in general categories risk clinical disruption from supply gaps.
What are common challenges in managing medical supply inventory turnover?
Medical supply inventory management carries several complications that standard retail inventory formulas do not account for.
Overstocking versus stockouts. The core tension in healthcare inventory is that excessively high turnover risks stockouts and compromises patient care. Chasing a high ratio without clinical context is dangerous. A facility that runs out of isolation gowns during a surge event has optimized itself into a crisis.
Consignment inventory distortion. Consignment inventory should be tracked separately because it skews turnover ratios and masks true holding costs. When vendor-owned stock sits in your storeroom, it inflates your apparent inventory without representing your actual capital exposure. Learn more about consignment inventory impacts before including it in your ratio calculations.
Category-specific replenishment velocity. Disposable PPE, surgical instruments, and diagnostic equipment each replenish at completely different rates. Treating them as one pool produces a ratio that accurately describes nothing.
Reverse logistics for reusable equipment. Reusable medical equipment adds complexity that standard turnover formulas miss entirely. Sterilization cycles, repair loops, and refurbishment timelines affect how much working capital is tied up at any given moment. Facilities that ignore reverse logistics consistently understate their true inventory needs.
Expiration-driven write-offs. Slow-moving inventory in healthcare does not just sit idle. It expires. Write-offs for expired supplies directly reduce COGS accuracy and distort future turnover calculations.
Pro Tip: Build a separate tracking register for consignment stock, reusable equipment in the refurbishment cycle, and items within 90 days of expiration. These three categories require different management responses than standard active inventory.
Proper medical equipment storage also affects turnover accuracy. Supplies stored incorrectly may expire faster or become unusable before consumption, creating phantom losses that distort your ratio.
How can healthcare facilities improve their inventory turnover ratio?
Improving the inventory turnover ratio in healthcare requires both technology and process discipline. The following five strategies produce measurable results.
Implement AI-driven demand forecasting. High-performing facilities now use AI-driven demand forecasting integrated with ERP systems to align inventory levels with clinical demand. This reduces both excess stock and emergency orders. AI forecasting tools analyze historical consumption patterns, seasonal demand shifts, and procedure schedules to generate accurate reorder points.
Integrate ERP systems with inventory management. Disconnected spreadsheets and manual counts produce inaccurate COGS and average inventory figures. ERP integration creates a single source of truth for consumption data, enabling accurate ratio calculations and faster response to demand changes.
Monitor turnover monthly and audit quarterly. Inventory turnover should be reviewed monthly in high-volume operations, with quarterly audits to catch stockouts and expired write-offs before they become costly. Monthly monitoring catches drift early. Quarterly audits provide the deeper category-level review that monthly snapshots miss.
Use blended vendor sourcing. High-volume buyers optimize procurement with blended vendor sourcing to improve turnover rates and reduce costs. Relying on a single supplier creates both pricing risk and supply disruption risk. Distributing orders across multiple qualified vendors improves negotiating leverage and supply continuity.
Automate replenishment for high-velocity items. Automated reorder triggers for fast-moving consumables like gloves, masks, and disposable gowns eliminate the manual review lag that causes both stockouts and panic-buying overstock. Set reorder points based on DOI targets, not gut instinct.
Each strategy compounds the others. AI forecasting without ERP integration produces recommendations that never reach the purchasing team. ERP integration without regular audits creates false confidence in data that has drifted from reality.
Key takeaways
The inventory turnover ratio is the single most actionable metric for reducing waste and protecting clinical availability in medical supply chains.
Point | Details |
Standard formula | Divide COGS by average inventory; convert to DOI by dividing 365 by the ratio. |
General healthcare benchmark | Target 3–5 turns per year; high-volume med-surg buyers target 4–6 turns annually. |
Category-specific targets | Apply separate benchmarks to consumables, implants, and reusables to avoid misleading blended ratios. |
Consignment and reverse logistics | Track consignment stock and reusable equipment separately to prevent ratio distortion. |
Technology and monitoring | Use AI forecasting with ERP integration and review turnover monthly to prevent stockouts and write-offs. |
Why chasing a high turnover ratio can backfire
I have watched supply chain teams celebrate a rising inventory turnover ratio while their clinical staff quietly built personal stashes of critical supplies in desk drawers. That is the clearest sign that the metric has been optimized in isolation from the people who actually use the supplies.
The ratio is a financial tool. Patient care is the operational reality. When those two things pull in opposite directions, the ratio always loses. A facility that cuts its PPE inventory to hit a 6.0 ratio and then scrambles during a demand spike has not improved its supply chain. It has just moved the cost from carrying charges to emergency procurement premiums and staff stress.
The facilities I have seen manage this well treat inventory turnover as one input among several, not as a scorecard. They run category-level reviews, involve clinical leads in reorder point decisions, and treat a sudden ratio spike as a warning sign rather than a win. A spike in turnover on a critical item often means someone is consuming more than planned, not that procurement is running efficiently.
The most underrated practice in healthcare inventory management is the cross-functional audit. When supply chain, finance, and clinical operations sit in the same room and review the same numbers quarterly, the blind spots disappear fast. No AI system replaces that conversation.
— QB
Medical supplies for healthcare facilities at Queenssurgical
Healthcare administrators who have their turnover metrics in order still need a reliable supplier to back up their reorder strategy.
Queenssurgical supplies hospitals, clinics, and surgical centers across the Americas with a full catalog of disposables, PPE, instruments, and equipment. From disposable face masks to isolation gowns, the platform offers both wholesale and retail purchasing with competitive pricing and consistent availability. Facilities managing tight DOI targets need a supplier that ships reliably and maintains stock on high-velocity items. Browse the full Queenssurgical catalog to source the consumables your turnover strategy depends on.
FAQ
What is the inventory turnover ratio in healthcare?
The inventory turnover ratio in healthcare measures how many times a facility cycles through its medical supply inventory in a given period. The standard formula is COGS divided by average inventory, with a benchmark of 3–5 turns per year for general healthcare facilities.
How do you calculate days of inventory on hand?
Divide 365 by the inventory turnover ratio. A turnover ratio of 4.0 equals approximately 91 days of inventory on hand, meaning current stock would last 91 days without replenishment.
Why is a very high inventory turnover ratio risky in healthcare?
A very high ratio signals lean stock levels that can lead to clinical stockouts. Excessively high turnover risks supply gaps that compromise patient care, particularly for critical or high-demand items.
Should consignment inventory be included in the turnover calculation?
No. Consignment inventory should be tracked separately because it skews the turnover ratio and hides true carrying costs. Including vendor-owned stock in your average inventory figure inflates the denominator and understates your actual capital exposure.
How often should healthcare facilities review inventory turnover?
High-volume operations should review turnover monthly, with deeper category-level audits conducted quarterly. Regular reviews catch expiration risks, demand shifts, and procurement inefficiencies before they become costly write-offs or stockouts.
Recommended
Comments